
Cardiovascular System
For ease of understanding, the development of the cardiovascular system can be summarized into the following categories which will each be discussed separately:
Formation of the heart tube
Formation of the chambers of the heart
Formation of blood vessels
Heart Tube
By week three of development, mesoderm in the region of what will become the cardiogenic field begins differentiating into a heart tube and pericardial cavity.
Blood islands appear near the cranial region of the embryo and unite to form an endocardial tube on either side of the developing embryo surrounded by myoblasts that will later differentiate into cardiac myoblasts. As embryonic folding begins taking place, as a result of lateral folding, the endocardial tubes on either side of the developing embryo will come together to form one heart tube while cephalocaudal folding will bring the developing heart from the cranial region to the thoracic region where it will continue to develop.
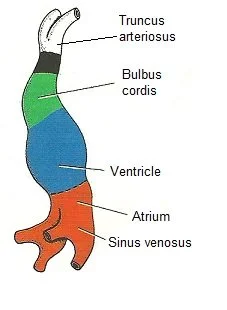
The heart tube begins begins with the following primitive parts that will later develop into structures within a mature heart:
Truncus arteriosus
Bulbus cordis
Primitive ventricle
Primitive atrium
Sinus venosus
Pattern of blood flow through the aforementioned structures can be summarized as:
Blood enters the heart tube through sinus venosus
It travels up to the primitive atrium
Followed by the primitive ventricles
Through bulbus cordis
Through truncus arteriosus
And out through the dorsal aortae

By the 23rd day of development, the heart tube begins looping on itself such that its various parts end up repositioning. This looping causes the bulbus cordis and truncus arteriosus to start moving downwards and to the right, this in turn causes the primitive ventricle to move upwards and to the left. As a result, the primitive atrium is pushed upwards and dorsally such that as it moves in this direction, it ultimately ends up above bulbus cordis and the primitive ventricle, while sinus venosus continues to feed blood into it. This looping occurs while the heart tube is contained within the pericardial cavity and it brings us closer to the final shape of mature heart. At this stage of development, the primitive atrium and ventricle are separated by an atrioventricular canal.
The following describe the primitive regions of a developing heart and the structures that they mature into:
Truncus arteriosus develops in the pulmonary trunk and ascending aorta
Bulbus cordis develops into the right ventricle as well as the outflow tracts of the heart
The primitive ventricle develops into the left ventricle
The primitive atrium develops into both the right and left atria
Sinus venosus develops into the coronary sinus and the inferior vena cava.
Chambers of the Heart

By week 5 of development, septa appear and compartmentalize the heart into its four chambers.
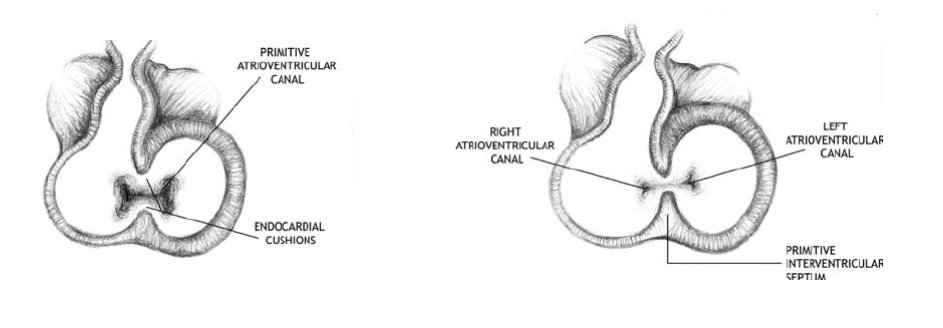
As a result of cell signaling, neural crest cells migrate to the region of the developing heart and give wise to endocardial cushions. During the 4th week of development, the anterior and posterior walls of the atrioventricular canal between the primitive atrium and primitive ventricle will begin to thicken and form the endocardial cushions. These endocardial cushions will continue to grow towards each other and will eventually be able to fuse together. By the 6th week of development, the endocardial cushions will unite, fuse, and separate the atrioventricular canal into 2 canals. This gives rise to the separation between the primitive atrium and primitive ventricle of the heart.
Following the fusion of the endocardial cushions, mesenchymal cells in this region will proliferate and give rise to the leaflets of primitive valves that maintain a connection with the walls of the primitive ventricle. Through development these connections to the primitive ventricle will develop into chordae tendinae with papillary muscles at their ventricular ends and the leaflets of the primitive valves will further develop into the right and left atrioventricular valves of the heart.

Simultaneously, a new ridge of tissue begins to proliferate in the roof of the primitive atrium known as septum primum which extends from the roof and grows towards the endocardial cushions. As septum primum grows towards the endocardial cushions an initial space exists between the two structures and this is known as ostium primum. This space will eventually close when septum primum reaches and fuses with the endocardial cushions. However, the fusion of these two structures gives rise to another space (this time in the central region of septum primum) and this is known as ostium secundum.
Next, a second ridge of tissue will begin to proliferate from the roof of the primitive atrium known as septum secundum. This new septum functions to block off ostium secundum, however, as it is unable to block off ostium secundum entirely, the gap that is left between septum secundum and ostium secundum is known as foramen ovale.
Foramen ovale works to shunt blood from the right atrium to the left atrium during fetal development, so oxygenated blood is able to enter systemic circulation while bypassing pulmonary circulation.
At the time of birth, the pressure changes that exist between the two atria of the heart (higher pressure in the left atrium) will push septum primum down against septum secundum effectively closing off foramen ovale as oxygenated blood no longer needs to bypass pulmonary circulation.

By the end of week four of development, a muscular interventricular septum begins to proliferate from the floor of the ventricular chamber towards the endocardial cushions. As the interventricular septum grows towards the endocardial cushions, an initial space exists between the two structures and this is known as an interventricular foramen. Eventually the endocardial cushions will extend inferiorly to complete the interventricular septum and this effectively closes off the interventricular foramen.
As such, a four chambered heart has been created.
Blood Vessels
The formation of blood vessels occurs in the following ways:
Vasculogenesis
Development of blood cell types of mesodermal cells
Mesodermal cells differentiate into hemangioblasts that will later differentiate into hematopoietic stem cells and angioblasts
These hematopoietic stem cells will form the blood cell types
Sites of vasculogenesis merge to form networks of blood vessels
Angiogenesis
Development of blood vessels from existing blood vessels
Endothelial cells proliferate to form new capillaries
At the end of week three of development, vasculogenesis results in the formation of blood islands near the cardiogenic field and notochord. These blood island unite to form the dorsal aortae, one on either side. The dorsal aortae will eventually give rise to the descending aorta as development progresses.
Between truncus arteriosus and the dorsal aortae will arise five pairs of aortic arches that develop within the pharyngeal arches and these will ultimately persist and various arteries in the head and neck region.
The fifth aortic arch however, will form a link between truncus arteriosus and the left dorsal aortae as the ductus arteriosus. This structure acts as a shunt between the pulmonary trunk and aorta and ensures that blood is able to bypass the lungs, instead moving directly from the right ventricle to the aorta during development. Ductus arteriosus persists as ligamentum arteriosum after birth.
The following summarize the embryonic vessels that exist during development:
Cardinal vessels
The cardinal veins drain the body of the embryo and while the posterior cardinal veins degenerate, the caudal cardinal veins remain as the sacral venous plexus and common iliac veins
The cardinal veins remain as the following structures:
Superior vena cava
Inferior vena cava
Azygos vein
Hemiazygos vein
Renal vein
Suprarenal vein
Gonadal vein
Umbilical vessels
The umbilical circulation describes the flow of blood between the chorion of the placenta and the embryo
The umbilical arteries carry poorly oxygenated blood to the placenta while the umbilical veins carry highly oxygenated blood to the heart during development
Ductus venosus is a shunt that allows the blood within the umbilical vein to bypass the liver and to enter the inferior vena cava
Ductus venosus will degenerate after birth and become ligamentum venosus
Proximal regions of the umbilical arteries remain as internal iliac and superior vesical arteries
Distal regions of the umbilical arteries remain as medial umbilical ligaments
The umbilical vein persists as ligamentum teres
Vitelline vessels
The vitelline circulation describes the flow of blood between the developing embryo and the yolk sac
Vitelline arties are branches of the dorsal aortae and they eventually degenerate except for the following branches:
Celiac trunk
Superior mesenteric artery
Inferior mesenteric artery
Vitelline veins will eventually contribute to the hepatic veins of the liver and the hepatic portal vein.
Fetal Blood Circulation
The following steps summarize the path of blood during fetal blood circulation:
Umbilical vein channels oxygenated blood from the placenta towards the liver
While some of the blood enters the liver, most of it is redirected by ductus venosus into the inferior vena cava
The oxygenated blood is then directed towards the right atrium of the heart
This oxygenated blood is shunted to the left atrium through foramen ovale
The oxygenated blood from the left atrium is then directed to the left ventricle before it is pushed through the aorta to enter systemic circulation
Poorly oxygenated blood enters the right atrium of the heart through the superior vena cava and the coronary sinus
This poorly oxygenated blood mixes a little with the well oxygenated blood in the left atrium thereby reduces the overall oxygen saturation of the blood
Poorly oxygenated blood from the right atrium will flow into the right ventricle of the heart and leave through the pulmonary artery, passing through ductus arteriosus to the descending aorta.
Clinical Notes:
Dextrocardia - this occurs when the heart develops on the right side of the thoracic cavity instead of the left and can often be associated with situs inversus.
Patent foramen ovale - this occurs when foramen ovale fails to close entirely which results in the continuous mixing of blood between the right and left atria.
Ventricular septal defect - this occurs when the interventricular septum fails to close entirely which results in the mixing of blood between the right and left ventricle.
Tetralogy of Fallot - this occurs when four congenital defects occur simultaneously, these include a ventricular septal defect, an overriding aorta, pulmonary stenosis, and right ventricular hypertrophy.
Patent Ductus Arteriosus - this occurs when ductus arteriosus fails to close at birth which results in the continuous mixing of blood between the aorta and pulmonary arteries.